Pleural Sarcoma: Symptoms, Causes, Diagnosis, Treatment, and Prognosis

Pleural sarcoma is a rare and aggressive type of cancer that develops in the pleura, the thin membrane that lines the lungs and the inside of the chest wall. Unlike more common pleural cancers such as Malignant Pleural Mesothelioma, pleural sarcoma arises from connective tissue cells rather than mesothelial cells. Because of its rarity, pleural sarcoma is often difficult to diagnose, and treatment typically requires a specialized, multidisciplinary approach.
This comprehensive article covers everything you need to know about pleural sarcoma, including its types, causes, symptoms, diagnosis, treatment options, and prognosis.
~What is Pleural Sarcoma?
Pleural sarcoma refers to a group of malignant tumors that originate from the soft tissues of the pleura. The pleura plays an essential role in lung function by producing lubricating fluid that allows smooth movement of the lungs during breathing. When sarcoma develops in this region, it can disrupt breathing and cause significant complications.
Because pleural sarcoma is extremely rare, it is often misdiagnosed as other pleural diseases, including mesothelioma or metastatic cancers. Early recognition and accurate diagnosis are crucial for improving outcomes.
~Types of Pleural Sarcoma
Pleural sarcoma is not a single disease but includes several types of soft tissue sarcomas that may affect the pleura.
1. Synovial Sarcoma of the Pleura
This is one of the most commonly reported pleural sarcomas. Despite its name, it does not originate from synovial tissue but from mesenchymal cells. It may present as a large chest mass.
2. Fibrosarcoma
Fibrosarcoma involves malignant fibroblasts and may develop in the pleura or surrounding chest structures.
3. Leiomyosarcoma
This type arises from smooth muscle cells and may originate from blood vessels in the pleura.
4. Undifferentiated Pleomorphic Sarcoma
Previously known as malignant fibrous histiocytoma, this is an aggressive tumor with no specific differentiation.
~Causes and Risk Factors
The exact cause of pleural sarcoma remains unknown. However, several factors may increase risk.
1. Genetic Mutations
Mutations in tumor suppressor genes and oncogenes can lead to uncontrolled growth of mesenchymal cells.
2. Radiation Exposure
Previous radiation therapy for cancers such as Breast Cancer or Lymphoma may increase the risk of developing secondary sarcomas in the chest.
3. Environmental Factors
Exposure to toxins and industrial chemicals may play a role, although evidence is limited.
Unlike mesothelioma, pleural sarcoma is not strongly linked to asbestos exposure.
~Symptoms of Pleural Sarcoma
Symptoms depend on tumor size, location, and whether the cancer has spread. Because the pleural cavity has space, tumors may grow large before causing symptoms.
Common Symptoms
Persistent chest pain
Shortness of breath
Chronic cough
Fatigue
Unexplained weight loss
Advanced Symptoms
Difficulty breathing
Pleural effusion (fluid accumulation)
Compression of lung tissue
Hoarseness
Difficulty swallowing
Pleural effusion can lead to severe breathing problems and often requires drainage.
~How is Pleural Sarcoma Diagnosed?
Diagnosing pleural sarcoma is challenging due to its rarity and similarity to other pleural tumors.
1. Medical History and Physical Examination
Doctors evaluate symptoms, occupational history, and previous radiation exposure.
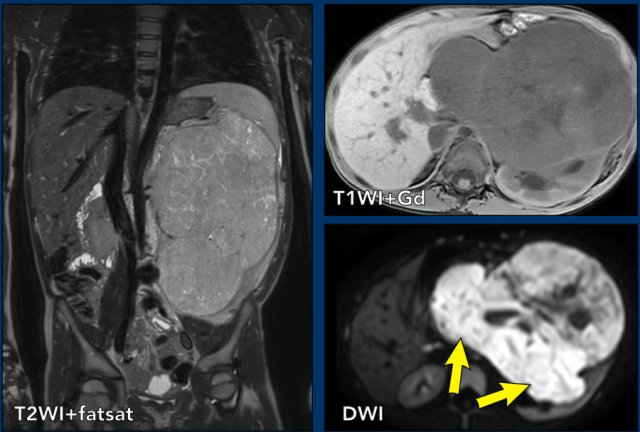
2. Imaging Tests
Key imaging studies include:
Chest X-ray
CT scan
MRI
PET scan
These help determine tumor size and spread.
3. Thoracentesis
Fluid from the pleural space may be examined, though it rarely confirms sarcoma.
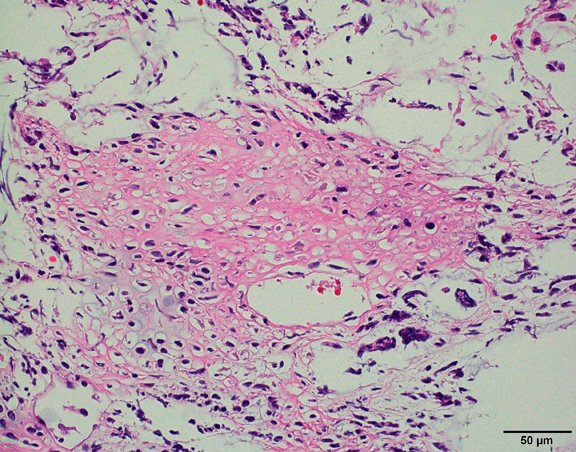
4. Biopsy
A core needle or surgical biopsy is required for definitive diagnosis.
5. Immunohistochemistry and Molecular Testing
These tests help differentiate pleural sarcoma from other cancers such as mesothelioma or metastatic tumors.
~Staging of Pleural Sarcoma
There is no universal staging system specific to pleural sarcoma, but staging is generally based on soft tissue sarcoma guidelines.
Stage I
Localized tumor.
Stage II
Larger tumor or involvement of nearby tissues.
Stage III
Spread to regional lymph nodes.
Stage IV
Metastasis to distant organs such as lungs, liver, or bones.
~Treatment Options for Pleural Sarcoma
Treatment depends on tumor type, stage, and patient health.
1. Surgery
Complete surgical removal is the cornerstone of treatment when possible. Procedures may include:
Tumor resection
Pleurectomy
Removal of affected lung tissue
Surgery offers the best chance for cure in early-stage disease.
2. Chemotherapy
Chemotherapy may be used:
Before surgery to shrink tumors
After surgery to prevent recurrence
In advanced disease
Common drugs include doxorubicin and ifosfamide.
3. Radiation Therapy
Radiation may be used as an adjunct to surgery or for symptom relief.
4. Targeted Therapy
Research is ongoing to identify molecular targets for personalized treatment.
5. Immunotherapy
Some patients may benefit from immune checkpoint inhibitors.
6. Clinical Trials
Due to the rarity of pleural sarcoma, clinical trials are an important option.
~Complications
Pleural sarcoma can lead to several complications:
Respiratory failure
Tumor compression of lungs
Recurrent pleural effusion
Metastasis
Severe pain
Early intervention helps reduce complications.
~Prognosis and Survival Rate
The prognosis varies depending on several factors.
Factors Affecting Prognosis
Tumor type
Stage at diagnosis
Surgical removal success
Patient health
Response to therapy
Localized tumors have a better outcome, while advanced disease has a poor prognosis.
~Difference Between Pleural Sarcoma and Mesothelioma
Although both affect the pleura, these cancers differ significantly.
| Feature | Pleural Sarcoma | Mesothelioma |
|---|---|---|
| Origin | Connective tissue | Mesothelial cells |
| Asbestos link | Rare | Strong |
| Frequency | Extremely rare | More common |
| Treatment | Similar to soft tissue sarcoma | Mesothelioma-specific |
Accurate diagnosis is essential for selecting the right treatment.
~Prevention and Risk Reduction
Because the exact cause is unclear, prevention focuses on general cancer risk reduction.
Key Measures
Avoid unnecessary radiation exposure
Limit chemical exposure
Maintain regular health checkups
Early evaluation of persistent chest symptoms
~Living with Pleural Sarcoma
Living with a rare cancer can be challenging.
Support Strategies
Psychological counseling
Support groups
Nutritional support
Pain management
Palliative care
These measures improve quality of life.
~Recent Advances in Research
Recent research focuses on:
Genetic profiling
Targeted therapies
Immunotherapy combinations
Early detection biomarkers
These developments offer hope for better survival.
~When to See a Doctor
Consult a healthcare provider if you experience:
Persistent chest pain
Shortness of breath
Unexplained weight loss
Recurrent pleural fluid
Early diagnosis improves treatment outcomes.
~Conclusion
Pleural sarcoma is a rare but aggressive cancer that requires early detection and specialized care. Because its symptoms mimic other pleural diseases, awareness and timely evaluation are crucial. Advances in surgery, chemotherapy, radiation, and immunotherapy continue to improve outcomes.
If you have persistent chest symptoms or risk factors, seek medical attention promptly. Ongoing research and clinical trials provide hope for better treatments and improved survival in the future.