Meningioma: Symptoms, Causes, Diagnosis, Treatment, and Prognosis
Meningioma is one of the most common types of brain tumors, accounting for nearly one-third of all primary brain and spinal tumors. Although most meningiomas are benign and slow-growing, some can become aggressive and require urgent medical intervention. Understanding the symptoms, causes, diagnosis, treatment options, and prognosis of meningioma is essential for patients, caregivers, and healthcare professionals.
~What Is a Meningioma?

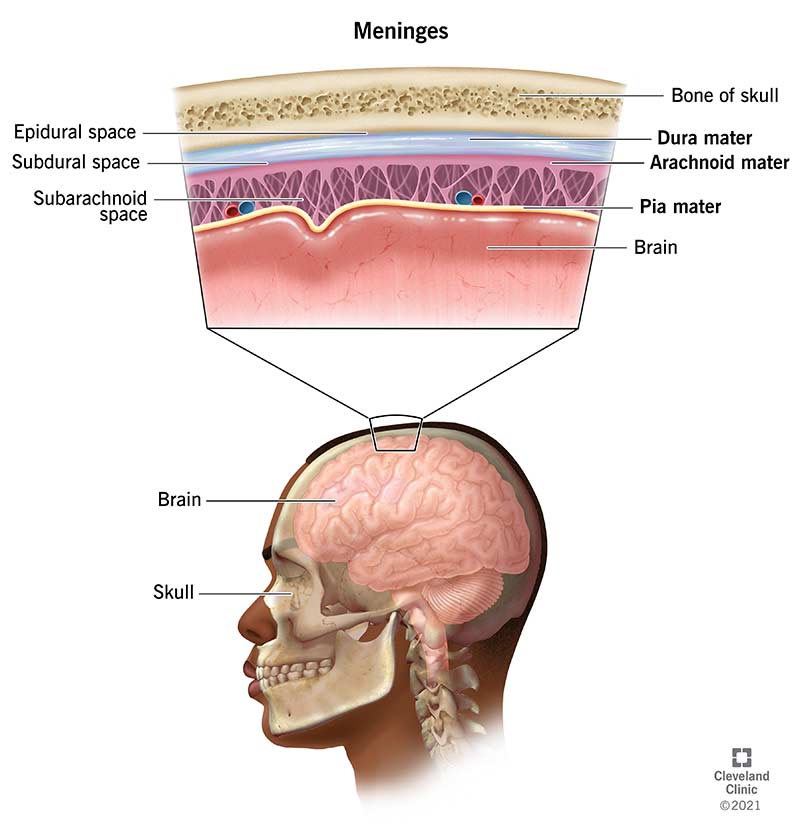

A meningioma is a tumor that develops from the meninges — the protective membranes that surround the brain and spinal cord. These tumors arise from arachnoid cap cells in the meninges and typically grow slowly over time.
Unlike many brain tumors that originate within brain tissue, meningiomas form on the outer surface of the brain. This means they may compress nearby brain structures rather than invade them directly.
Key Facts About Meningioma
Accounts for about 30–40% of primary brain tumors
More common in women than men
Most frequently diagnosed in adults over age 40
Usually benign (non-cancerous)
Can occur in the brain or spinal cord
~Types of Meningioma
Meningiomas are classified based on their location and histological features.
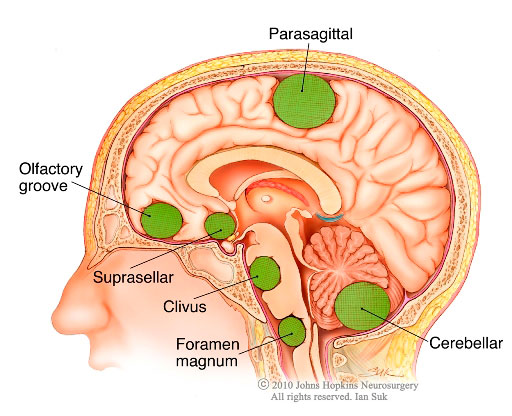
Based on Location
Convexity Meningioma – Found on the brain’s outer surface
Skull Base Meningioma – Located at the base of the skull
Parasagittal Meningioma – Near the superior sagittal sinus
Spinal Meningioma – Develops in the spinal canal
Olfactory Groove Meningioma – Near the nasal cavity
Based on WHO Grade
The World Health Organization (WHO) classifies meningiomas into three grades:
Grade I (Benign) – Slow-growing, least aggressive (80–85% of cases)
Grade II (Atypical) – Faster-growing, higher recurrence risk
Grade III (Anaplastic/Malignant) – Rare but aggressive
~Causes of Meningioma
The exact cause of meningioma remains unclear, but several risk factors have been identified.
1. Genetic Mutations
Mutations in the NF2 gene (Neurofibromatosis Type 2) are strongly associated with meningiomas. Patients with NF2 have a higher risk of developing multiple tumors.
2. Radiation Exposure
Previous exposure to radiation therapy, especially to the head during childhood, significantly increases the risk.
3. Hormonal Influence
Meningiomas are more common in women, suggesting a hormonal link. Some tumors contain progesterone receptors, and growth may accelerate during pregnancy.
4. Age
Risk increases with age, particularly after 40.
5. Obesity
Studies suggest a possible association between obesity and increased meningioma risk.
~Symptoms of Meningioma

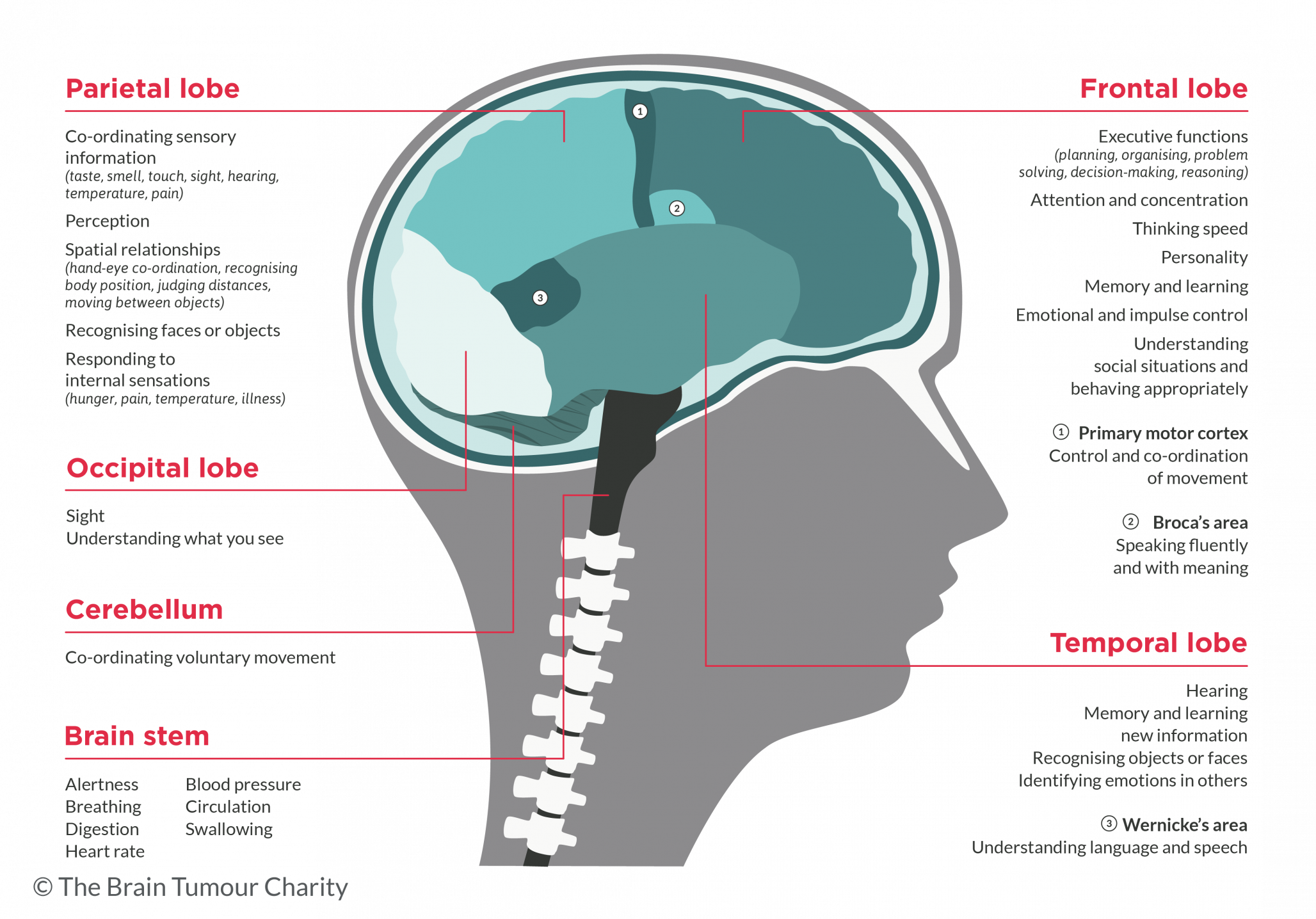


Symptoms depend on the tumor’s size and location. Because meningiomas grow slowly, symptoms may develop gradually.
Common Symptoms
Persistent headaches
Seizures
Vision changes (blurred or double vision)
Hearing loss
Memory problems
Weakness in arms or legs
Personality or behavioral changes
Spinal Meningioma Symptoms
Back pain
Difficulty walking
Numbness or tingling
Bowel or bladder dysfunction
Some small meningiomas may be discovered incidentally during imaging for unrelated conditions.
~How Is Meningioma Diagnosed?
Diagnosis typically involves imaging studies and sometimes biopsy.
1. MRI (Magnetic Resonance Imaging)
MRI is the gold standard for diagnosing meningioma. It provides detailed images of tumor size, location, and effect on surrounding structures.
2. CT Scan
Useful for detecting bone involvement or calcifications.
3. Biopsy
A biopsy may be performed during surgery to determine the tumor grade.
4. Neurological Examination
Doctors assess reflexes, coordination, vision, and cognitive function.
~Treatment Options for Meningioma
Treatment depends on tumor size, location, grade, symptoms, and overall health of the patient.
1. Watchful Waiting (Active Surveillance)
For small, asymptomatic meningiomas, doctors may recommend regular MRI scans without immediate treatment.
2. Surgery



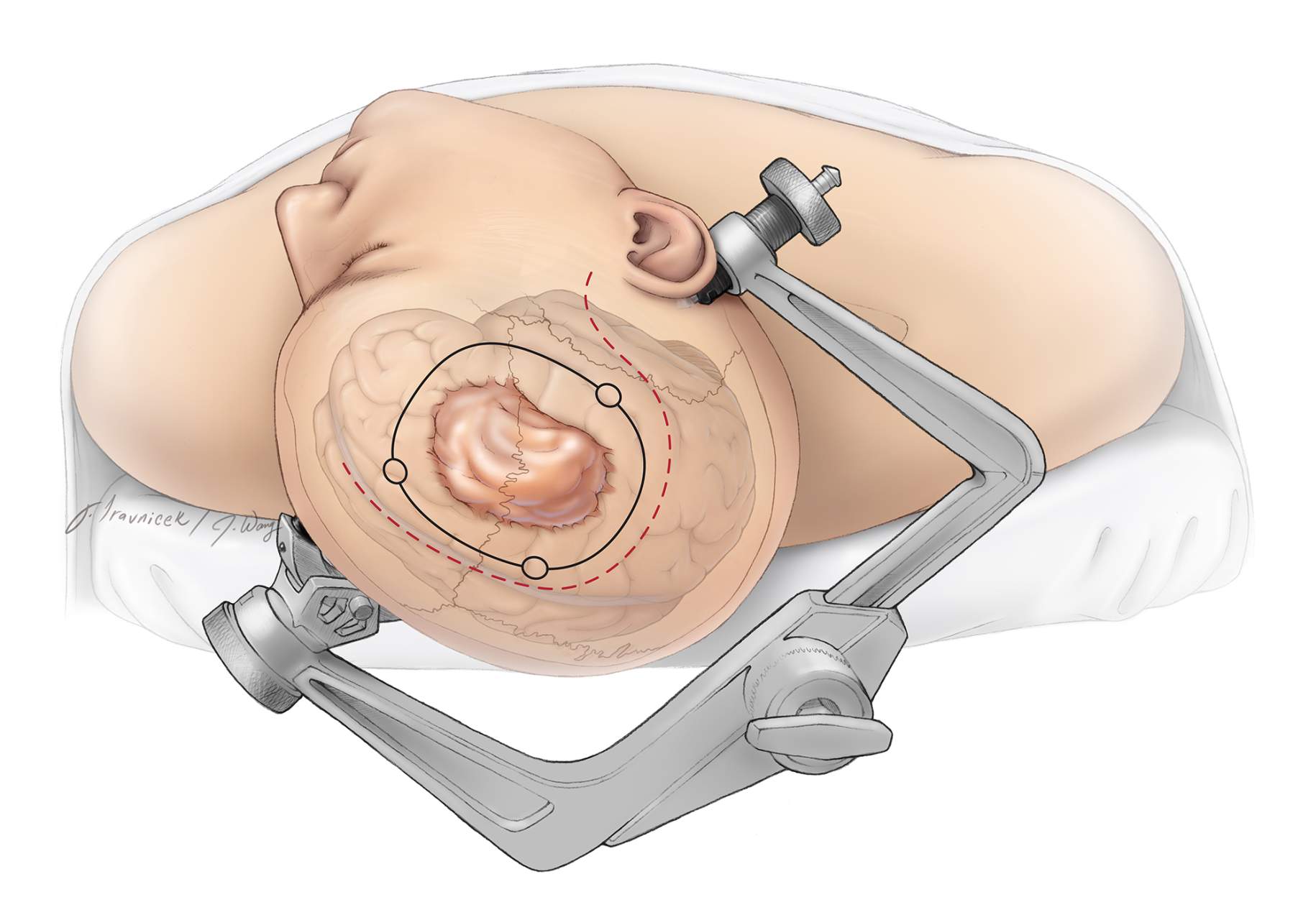
Surgical removal is the primary treatment for symptomatic meningiomas.
Goal: Remove as much of the tumor as safely possible.
Complete removal reduces recurrence risk. However, tumors near critical brain structures may only be partially removed.
Risks of Surgery
Infection
Bleeding
Neurological deficits
Swelling
3. Radiation Therapy
Used when:
Surgery is not possible
Tumor is partially removed
Tumor recurs
Types include:
External beam radiation
Stereotactic radiosurgery (e.g., Gamma Knife)
4. Chemotherapy
Rarely used for benign meningiomas but may be considered for aggressive or recurrent tumors.
5. Targeted Therapy & Clinical Trials
New research focuses on molecular-targeted therapies, immunotherapy, and genetic-based treatments.
~Recovery After Meningioma Surgery
Recovery varies depending on tumor location and patient health.
Typical Recovery Timeline
Hospital stay: 3–7 days
Return to work: 4–8 weeks
Full recovery: Several months
Physical therapy, speech therapy, or occupational therapy may be required.
~Meningioma Recurrence Rates
Recurrence depends on tumor grade and completeness of removal.
Grade I: 5–20% recurrence
Grade II: 30–40% recurrence
Grade III: Up to 50–80% recurrence
Regular follow-up MRI scans are essential.
~Meningioma Survival Rate
Survival rates vary by grade.
5-Year Survival Rate
Grade I: Over 90%
Grade II: 75–85%
Grade III: 50–60%
Early diagnosis significantly improves outcomes.
~Complications of Meningioma
If untreated, large tumors can cause:
Increased intracranial pressure
Brain herniation
Permanent neurological damage
Post-treatment complications may include cognitive changes or motor weakness.
~Can Meningioma Be Prevented?
There is no guaranteed way to prevent meningioma. However:
Avoid unnecessary radiation exposure
Maintain a healthy weight
Seek early medical evaluation for persistent neurological symptoms
Genetic counseling may help individuals with NF2.
~Living With Meningioma
A meningioma diagnosis can be overwhelming, but many patients live normal, healthy lives — especially with Grade I tumors.
Tips for Patients
Attend all follow-up appointments
Report new symptoms immediately
Maintain a healthy lifestyle
Seek emotional support or counseling
Support groups and patient advocacy organizations can provide guidance and reassurance.
~Advances in Meningioma Research (2026 Update)
Recent research highlights:
Genetic profiling for personalized treatment
Improved radiation precision techniques
AI-assisted imaging for earlier detection
Novel immunotherapy trials
These advances are improving outcomes, especially for atypical and malignant meningiomas.
~Frequently Asked Questions (FAQs)
Is meningioma cancer?
Most meningiomas are benign. However, atypical and anaplastic forms can be cancerous.
How fast does meningioma grow?
Many grow slowly over years. Some aggressive types grow rapidly.
Is meningioma life-threatening?
Small benign tumors may not be life-threatening. Large or malignant tumors can become serious if untreated.
Can meningioma shrink on its own?
Rarely. Most require monitoring or treatment.
Does meningioma run in families?
Most cases are sporadic, but genetic disorders like NF2 increase risk.
~When to See a Doctor
Seek immediate medical attention if you experience:
Sudden seizures
Severe persistent headaches
Vision loss
Weakness on one side of the body
Early intervention improves prognosis.
~Conclusion
Meningioma is the most common primary brain tumor, often benign and manageable with proper medical care. While many cases require only monitoring, others may need surgery or radiation therapy. Advances in medical technology and research are continuously improving treatment outcomes and survival rates.
If you or a loved one has been diagnosed with meningioma, consult a neurologist or neurosurgeon to develop a personalized treatment plan. Early detection, appropriate intervention, and consistent follow-up are key to long-term health and recovery.




No comments:
Post a Comment