Myoepithelial Carcinoma: Symptoms, Causes, Diagnosis, Treatment & Prognosis
Myoepithelial carcinoma is a rare and potentially aggressive malignant tumor that arises from myoepithelial cells — specialized cells found in glands such as the salivary glands, sweat glands, and breast tissue. Although uncommon, this cancer can develop in both soft tissue and visceral organs and may behave aggressively depending on its location and molecular characteristics.
Because myoepithelial carcinoma is rare, it is often misdiagnosed or confused with other soft tissue or salivary gland tumors. Early recognition and accurate histopathological diagnosis are crucial for effective treatment.
This comprehensive guide covers myoepithelial carcinoma symptoms, causes, risk factors, diagnosis, treatment options, recurrence risk, and survival rates.
~What Is Myoepithelial Carcinoma?
Myoepithelial carcinoma (also called malignant myoepithelioma) is a cancer that originates from myoepithelial cells. These cells normally surround glandular structures and help expel secretions.
It can occur in:
Salivary glands (most common site)
Soft tissues
Skin
Breast
Lung (rare)
Bone (rare)
When it arises in salivary glands, it is classified under salivary gland malignancies. It may develop on its own or evolve from a benign tumor such as pleomorphic adenoma.
~Common Locations of Myoepithelial Carcinoma
1. Salivary Glands (Most Common)
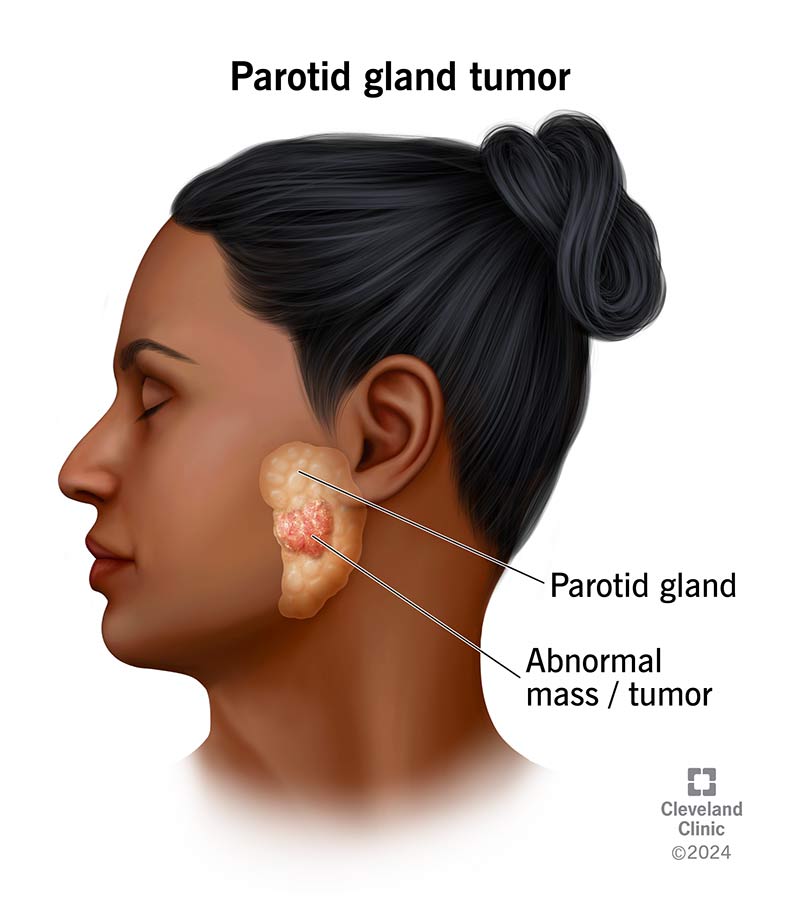

 The parotid gland is the most frequently affected salivary gland. Tumors may also arise in minor salivary glands located in the palate and oral cavity.
The parotid gland is the most frequently affected salivary gland. Tumors may also arise in minor salivary glands located in the palate and oral cavity.
Symptoms include:
Painless swelling near the jaw or ear
Facial nerve weakness (advanced cases)
Difficulty swallowing (rare)
2. Soft Tissue Myoepithelial Carcinoma



Soft tissue forms may occur in:
Extremities (arms and legs)
Trunk
Deep muscle tissue
These tumors may present as:
Slowly enlarging mass
Firm or rubbery lump
Pain (if compressing nerves)
3. Skin (Cutaneous Myoepithelial Carcinoma)
Rarely, myoepithelial carcinoma can arise in the skin, often confused with other skin cancers.
~Symptoms of Myoepithelial Carcinoma
Symptoms depend on tumor location.
General Symptoms
Growing mass
Local pain
Swelling
Firm nodular lesion
Salivary Gland Symptoms
Jaw or neck lump
Facial asymmetry
Numbness or facial paralysis
Soft Tissue Symptoms
Deep tissue swelling
Restricted movement
Tenderness
Some tumors remain painless for months, leading to delayed diagnosis.
~Causes and Risk Factors
The exact cause of myoepithelial carcinoma is not fully understood. However, several factors may contribute.
1. Genetic Alterations
Some tumors show EWSR1 gene rearrangements. These molecular abnormalities help confirm diagnosis.
2. Malignant Transformation
In some cases, myoepithelial carcinoma develops from a benign tumor such as:
Pleomorphic adenoma
This transformation increases aggressiveness.
3. Radiation Exposure
Prior radiation therapy to the head and neck may increase risk.
4. Age
Most cases occur in adults between 30 and 60 years, but it can affect children as well.
~How Is Myoepithelial Carcinoma Diagnosed?
Due to its rarity, diagnosis requires specialized pathological evaluation.
1. Clinical Examination
A persistent mass that continues to enlarge should raise suspicion.
2. Imaging Studies
Doctors may use:
MRI (preferred for soft tissue tumors)
CT scan
Ultrasound
Imaging helps assess:
Tumor size
Local invasion
Lymph node involvement
3. Biopsy
A biopsy is essential for diagnosis.
Types include:
Core needle biopsy
Excisional biopsy
Fine needle aspiration (salivary gland cases)
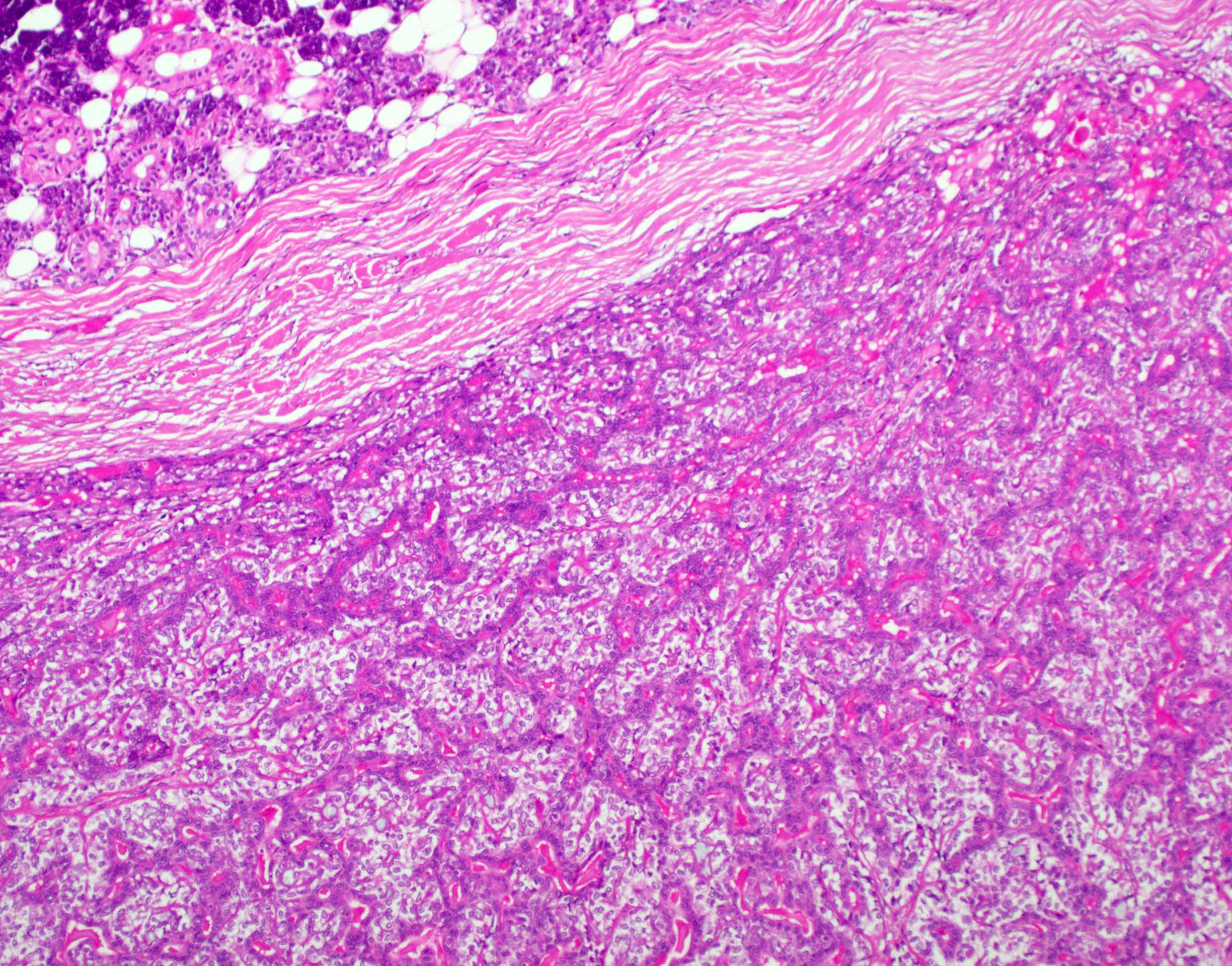
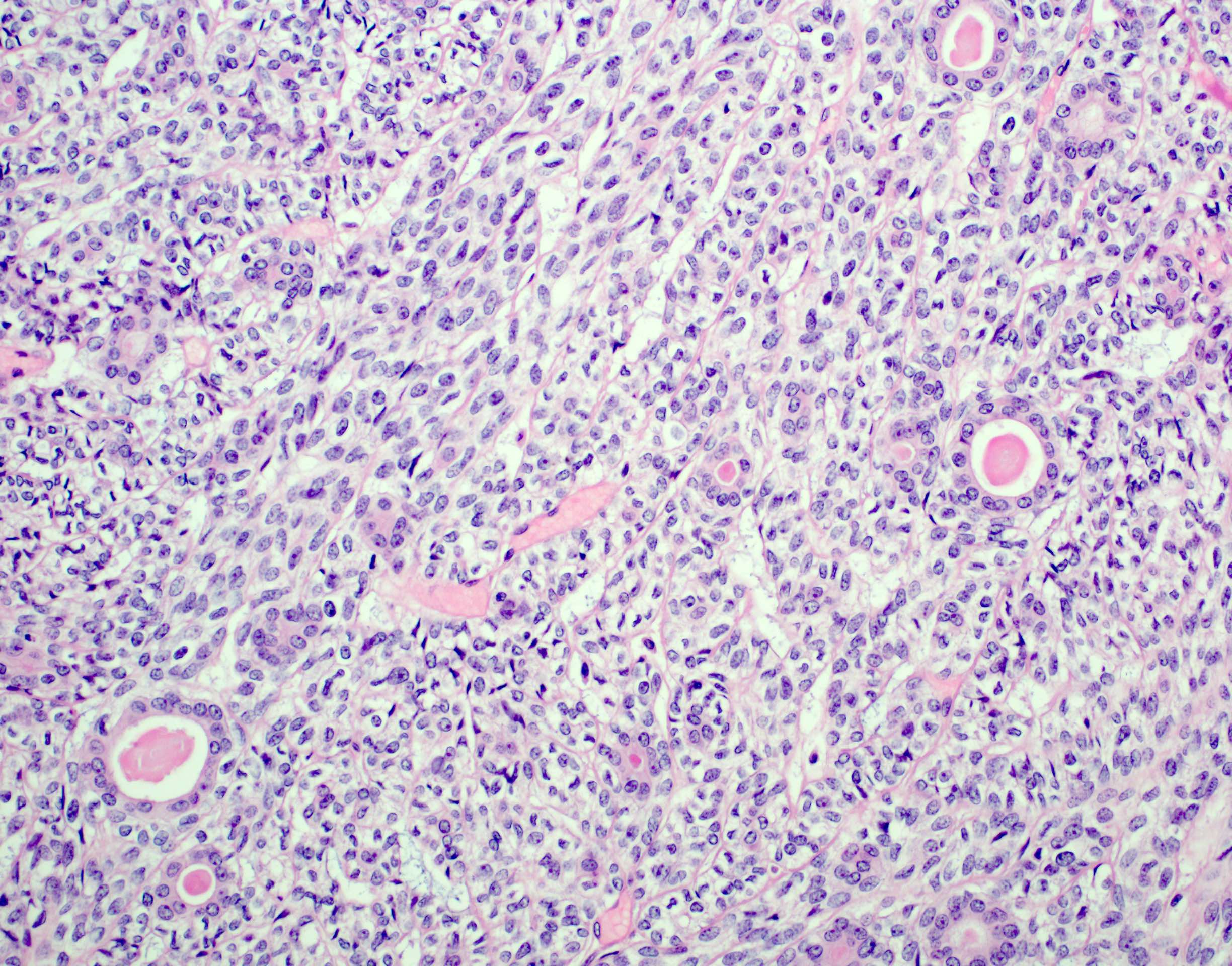
4. Histopathology
Under the microscope, myoepithelial carcinoma shows:
Cellular atypia
High mitotic activity
Infiltrative growth
Variable morphology (spindle, epithelioid, clear cell, or plasmacytoid cells)
5. Immunohistochemistry
Tumor cells often express markers such as:
Cytokeratin
S100 protein
Calponin
Smooth muscle actin (SMA)
GFAP (occasionally)
These markers confirm myoepithelial differentiation.
~Staging of Myoepithelial Carcinoma
Staging depends on:
Tumor size
Local invasion
Lymph node involvement
Distant metastasis
Soft tissue tumors are staged using sarcoma staging systems.
Common metastatic sites include:
Lungs
Lymph nodes
Bone
Liver
~Treatment of Myoepithelial Carcinoma
Treatment depends on tumor location, size, and spread.
1. Surgical Removal (Primary Treatment)
Complete surgical excision with clear margins is the main treatment.
For salivary gland tumors:
Parotidectomy (partial or total)
Possible facial nerve preservation or reconstruction
For soft tissue tumors:
Wide local excision
Clear surgical margins significantly reduce recurrence risk.
2. Radiation Therapy
Radiation may be recommended when:
Margins are positive
Tumor is large
High-grade features are present
Local recurrence occurs
3. Chemotherapy
Chemotherapy is considered in:
Metastatic disease
Unresectable tumors
Recurrent aggressive cases
There is no standardized chemotherapy protocol due to rarity.
4. Targeted Therapy and Research
Molecular profiling may guide targeted therapy in advanced cases, particularly when EWSR1 rearrangement is identified.
Clinical trials are ongoing for rare sarcoma subtypes.
~Recurrence Risk
Myoepithelial carcinoma has a moderate to high recurrence rate, particularly in:
Incomplete excision
High-grade tumors
Deep soft tissue locations
Recurrence may occur locally or as distant metastasis.
Long-term follow-up is essential, often for 5–10 years.
~Prognosis and Survival Rate
Prognosis depends on several factors:
Favorable Factors
Small tumor size
Complete surgical excision
Low mitotic rate
Poor Prognostic Factors
Large tumor
High-grade histology
Metastasis at diagnosis
Positive margins
Overall 5-year survival rates vary widely (approximately 50–80%), depending on stage and location.
Soft tissue myoepithelial carcinomas may behave more aggressively than salivary gland tumors.
~Differential Diagnosis
Because of its varied appearance, myoepithelial carcinoma may be confused with:
Epithelioid sarcoma
Synovial sarcoma
Metastatic carcinoma
Clear cell sarcoma
Malignant peripheral nerve sheath tumor
Accurate pathology review is crucial.
~Living With Myoepithelial Carcinoma
Patients may require multidisciplinary care involving:
Surgical oncologist
Radiation oncologist
Pathologist
Head and neck specialist (salivary tumors)
Rehabilitation may include:
Physical therapy (extremity tumors)
Facial nerve therapy (parotid tumors)
Psychological support
~Follow-Up and Monitoring
Regular follow-up visits are critical.
Monitoring typically includes:
Physical exams every 3–6 months (first 2 years)
Imaging as needed
Chest scans to detect lung metastasis
Early detection of recurrence improves outcomes.
~When to See a Doctor
Seek medical evaluation if you notice:
A growing mass in the neck, jaw, or limbs
Persistent painless swelling
Facial nerve weakness
Recurrent salivary gland lump
Deep tissue mass that continues enlarging
Prompt biopsy improves early detection.
~Frequently Asked Questions
Is myoepithelial carcinoma rare?
Yes, it is a rare cancer affecting both salivary glands and soft tissue.
Is it aggressive?
It can be aggressive, especially high-grade or metastatic forms.
Can it spread?
Yes, it may metastasize to lungs, lymph nodes, or bone.
Is it curable?
Early-stage tumors treated with complete surgical excision have better outcomes.
~Key Takeaways
Myoepithelial carcinoma is a rare malignant tumor of glandular and soft tissue origin.
Most commonly affects salivary glands and extremities.
Diagnosis requires biopsy and immunohistochemical testing.
Surgery is the primary treatment.
Recurrence and metastasis are possible.
Long-term monitoring is essential.
~Conclusion
Myoepithelial carcinoma is a rare but potentially serious malignancy that requires prompt diagnosis and aggressive management. Its variable presentation and resemblance to other tumors make expert pathological evaluation essential.
Complete surgical removal remains the cornerstone of treatment, often combined with radiation therapy in high-risk cases. Due to the possibility of recurrence and metastasis, long-term follow-up is critical.
Awareness of symptoms and early medical evaluation can significantly improve prognosis and survival outcomes.




No comments:
Post a Comment